Beyond the Clinic Walls: Rethinking HIV Prevention Through Rural Drug Shops
Written by: Nomujuni Natukwatsa, Florence Mwangwa, and Collins Ampaire | Team Gamba Link, Uganda
What if the first conversation about HIV prevent ion didn’t happen in a hospital but in a small drug shop down the road?
In many rural communities across Uganda, young people rarely walk into hospitals to ask about sexual health products. Instead, they rely on community drug shops and trusted community care providers as their first point of contact for sexual health needs which may include HIV prevention services. Yet these accessible and trusted spaces are often excluded from formal HIV prevention strategies.
Our inspiration
The INSPIRE Designathon provided a platform for us to develop the Gamba Link project. Gamba means to speak, tell or address in Bantu languages in Uganda. Our project aims to onboard community medicine providers by introducing them to structured HIV prevention information in order to support them to speak to young people about accessing biomedical HIV prevention products. The Gamba Link project developed the PREP-Go toolkit, a tool box of familiar communication tools to support community medicine providers like drug shop attendants to initiate youth-friendly, non-judgmental conversations about using HIV prevention products and link adolescents and young adults (AYAs) to peer navigators for PrEP services at formal health facilities.
The challenge that birthed Gamba Link
Pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP) are proven, effective HIV prevention tools. However, uptake among adolescents and young adults (15–24 years), particularly in rural areas, remains low. Young adolescents who are just beginning their sexual health journeys (15-20 years) are particularly vulnerable. Structural barriers such as low knowledge, fear of discussing sexual related matter with authority figures, stigma, limited youth-friendly services, and weak referral systems continue to stand in the way.
Through community engagement and prior evidence, we learned an important insight — many rural youth do go and seek sexual health products from trusted community drug shops. These spaces are informal, familiar, and discreet. Despite this, drug shop attendants are rarely equipped with the confidence, language, or tools to discuss sensitive topics like HIV prevention.
This gap presented both a challenge and an opportunity.
Turning community drug shops into gateways for HIV prevention access
We designed PREP-Go, a structured communication toolkit that supports drug shop attendants to confidently and non-judgmentally initiate conversations about accessing HIV prevention with the help of age appropriate support through peer navigators, who provide PrEP in formal health services.
Because community drug shops are not yet authorized to prescribe PrEP, we believe PREP-Go toolkit enables them to participate in HIV prevention actively by:
- Arousing curiosity about PrEP products
- Sharing accurate, stigma-free PrEP information
- Providing a clear referral pathway to supportive PrEP providers
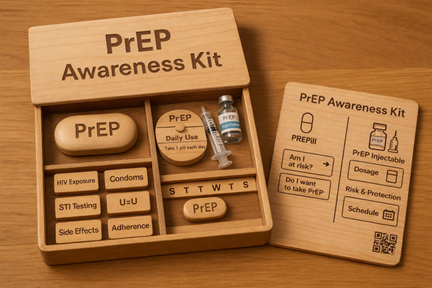
The toolkit includes a simple poster with visual information on who needs PrEP and how to access it, flash cards with PrEP choices, and a short, animated video to watch privately or share with acquaintances. All participating shops will have the name and phone contact of the nearest PrEP peer navigator.
Designing with, not for, the community
We engaged multiple stakeholders from the start: adolescents and young adults, drug shop attendants, and peer navigators. Their lived experiences helped shape every design decision.
Drug shop attendants told us they often wanted to help young people but feared saying the wrong things which would scare away their customers. Youth shared that they valued confidentiality, discretion, and respectful communication more than medical expertise. Peer navigators emphasized the importance of building trust in the communities. These insights informed a key design principle: keep it simple, visual, supportive, and scalable.

Testing the solution in the real world
The PREP-Go tool kit is being tested through a qualitative pilot study in four rural community pharmacies and drug shops in Lyantonde District of southwestern Uganda. The study uses a pre- and post-intervention design to assess feasibility, acceptability, fidelity, and sustainability.
To understand how the toolkit works in practice, we are collecting data from:
- Drug shop attendants who are using the toolkit
- Peer navigators supporting referrals
- Trained youth mystery clients observing real interactions
By combining focus group discussions, in-depth interviews, and mystery client visit reports, we aim to capture honest feedback on how youth experience PrEP conversations in these informal health settings.
Why this matters for youth
Young people in rural communities face a disproportionate risk of HIV due to social vulnerability, early sexual debut, limited access to services, and stigma. By bringing youth acceptable PrEP conversations closer to where youth already are, the PREP-Go toolkit helps normalize HIV prevention conversations even in commercial spaces and reduces missed opportunities for seeking these services.
Equally important, the project builds youth leadership. Peer navigators and mystery clients gain skills in advocacy, communication, and community engagement — strengthening local capacity beyond the project lifespan.
Looking ahead
We envision a world where talking about HIV prevention is as normal, stigma-free, and accessible as buying pain relief medicine at a drug shop.
Through the PREP-Go toolkit, we test if well-designed communication tools can unlock big changes in how communities approach HIV prevention. With continued collaboration, learning, and refinement, this model has the potential to transform rural HIV prevention across Uganda and similar settings.
Innovation does not always require new buildings or complex technologies. Sometimes, it starts with the right tools sparking a conversation among willing people.








