Written by: Julianah Adebisi and Miracle Adesina | IMPACT Team, Nigeria.
We didn’t notice it at first, but something had changed.
Just weeks earlier, Zainab had become a major driving force behind HIV outreach in the camp. Young people were showing up to discussions. Her peers listened, showed up, and stayed engaged.

“Zainab” engaging her peers during an HIV outreach session in the camp. Peer trust is often the foundation of youth health programs.
There was energy, the kind you hope for when working with peer-led models.
Then, a personal conflict disrupted those relationships, and with it, the flow of new participants into the program.
Our most successful outreach channel had slowed to a halt.
That moment made us rethink what we thought we understood about peer-led models, especially in displacement settings.
Why we chose a peer-led approach
Young people often learn about sex, relationships, and risk from their peers long before they encounter formal health services. Peer-led outreach taps into these existing social networks. The logic is simple, versatile, and compelling: young people trust their peers, understand each other’s realities, and communicate information in ways that feel relatable.
For the Innovative Mobilization and Participatory Action for Community Transformation (IMPACT) project, this approach felt especially appropriate as we worked with young people living in Internally Displaced Persons (IDP) camps in Nigeria.
We trained a small group of youth champions and encouraged them to reach out to peers in their own social circles: friends, neighbours, and classmates at camp. It was a snowball approach. Each young person could bring others.
It seemed to work; we were gaining momentum.
Where we hit a wall
One champion stood out. Zainab was motivated, well-respected, and committed to the project. Through her efforts, we saw a noticeable increase in participation. Her peers listened to her. They showed up. Momentum began to build.
Without realizing it, we began to rely heavily on her network.
So, when conflict emerged from within her circle, the impact rippled outward. She stepped back from active recruitment. The peers she had mobilized became less engaged. New participants stopped coming.
At first, it felt like a setback. We had invested in training. We had seen progress, and now the progress was slowing.
However, with reflection, we realized that this wasn’t a failure of Zainab or her peers.
It was a gap in our project design.
What this taught us about peer networks
Peer-led models often assume that social networks are stable. In some communities, that may be true. However, in IDP camps, relationships live under constant strain.
Young people are navigating economic stress, family trauma, uncertainty about the future and competition for limited resources. These pressures do not stay outside the room when we hold HIV sessions; they affect how young people relate to each other.
In that environment, small disagreements can grow quickly.
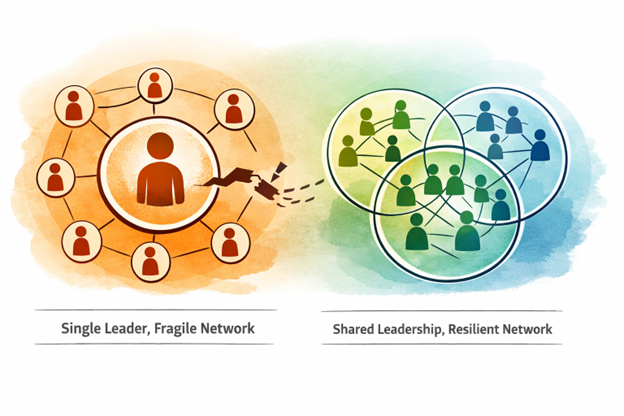
Emotional strain is high, and when leadership is concentrated in one person, a single strained relationship can stall momentum.
What slowed our outreach was not resistance to HIV education. It was the fragility of relationships in a high-stress setting.
An illustration of shared leadership in youth outreach. Programs are strongest when responsibility is distributed.
An illustration of shared leadership in youth outreach. Programs are strongest when responsibility is distributed.
Rethinking how we support youth champions
The situation compelled us to reassess our support for young people who assume leadership roles in health programs.
Being a youth champion is more than delivering information; it means managing friendships, expectations, and sometimes tension, all while mobilizing others.
From this experience, we learned that peer-led models work better when leadership is distributed, rather than concentrated. Recruiting champions in clusters makes the program less vulnerable to the ups and downs of a single relationship.
We also learned that conflict is not a disruption to community work but a part of it. Creating space for early conversations, mentorship, and mediation matters more than we initially realized.
Designing youth health programs for real-life complexity
In displacement settings, health education competes with urgent daily needs influenced by economic pressure, emotional stress, and unstable social relationships, all of which affect how young people engage with HIV prevention.
Peer-led approaches need to be designed with flexibility and empathy, recognizing that health is only one part of what young people are dealing with every day.
Our experience reminded us that effective youth health programming in humanitarian contexts requires careful design, including:
- Avoiding over-reliance on one champion
- Investing in supporting relationships, not just training
- Linking HIV outreach with livelihood support, psychosocial services, and other programs that respond to young people’s everyday realities
Moving forward
The setback in our recruitment was not the end of the story.
It pushed us to distribute leadership more intentionally, to check in more frequently with our youth champions, and to treat relational dynamics as part of program design.
Peer power remains one of the strongest tools in youth HIV prevention.
However, these peer-led models are only as strong as the relationships that sustain them.

Youth champions and participants during outreach. Peer power continues, strengthened by shared responsibility.